CPT Excision Guidelines: Coding Lesion Removal for the CPC Exam
By CPCPrep Team ·
CPT excision guidelines: coding lesion removal for the CPC exam
The three variables that determine the code
Every excision code comes down to three inputs. Get all three right and you land on the correct code. Miss one and you will be wrong in a way that looks plausible, which is exactly how the CPC exam is designed.
Benign vs malignant: two completely different code ranges
Benign lesions use codes 11400-11471. Malignant lesions use 11600-11646. These ranges do not overlap and do not share codes. The operative report or pathology note will specify benign or malignant. If the scenario does not state a diagnosis, look for contextual clues: melanoma, basal cell carcinoma, and squamous cell carcinoma are malignant. Cysts, lipomas, and nevi are benign unless stated otherwise.
This distinction matters for more than just picking the right range. Malignant lesions typically require wider surgical margins to achieve complete excision, which changes the excised diameter calculation. More on that below.
Anatomical location: how CPT groups body areas
CPT does not code excision by individual body part. It uses three location groups that appear in both the benign and malignant ranges:
- Trunk, arms, legs
- Scalp, neck, hands, feet, genitalia
- Face, ears, eyelids, nose, lips, mucous membrane
Each group has its own row of codes across six diameter ranges. A 1.5 cm lesion on the arm codes differently from a 1.5 cm lesion on the face. Read the location in the scenario carefully: “right cheek” is face, “right hand dorsum” is scalp/neck/hands, “left thigh” is trunk/arms/legs.
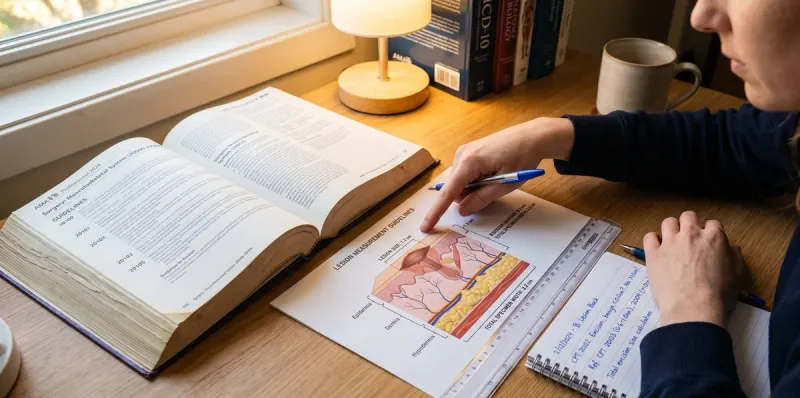
Excised diameter: not the lesion size alone
This is where most exam errors happen. The excised diameter is not the lesion size. It is the lesion’s greatest clinical diameter plus the narrowest surgical margin required for complete excision on each side.
The excised diameter is what gets measured and documented in the operative report. The CPC exam will sometimes give you the lesion size and the margin separately, requiring you to calculate the excised diameter yourself.
CPT code ranges (11400-11646): quick reference
Benign excision codes (11400-11471)
| Location | 0.5 cm or less | 0.6-1.0 cm | 1.1-2.0 cm | 2.1-3.0 cm | 3.1-4.0 cm | Over 4.0 cm |
|---|---|---|---|---|---|---|
| Trunk, arms, legs | 11400 | 11401 | 11402 | 11403 | 11404 | 11406 |
| Scalp, neck, hands, feet, genitalia | 11420 | 11421 | 11422 | 11423 | 11424 | 11426 |
| Face, ears, eyelids, nose, lips, mucous membrane | 11440 | 11441 | 11442 | 11443 | 11444 | 11446 |
Malignant excision codes (11600-11646)
| Location | 0.5 cm or less | 0.6-1.0 cm | 1.1-2.0 cm | 2.1-3.0 cm | 3.1-4.0 cm | Over 4.0 cm |
|---|---|---|---|---|---|---|
| Trunk, arms, legs | 11600 | 11601 | 11602 | 11603 | 11604 | 11606 |
| Scalp, neck, hands, feet, genitalia | 11620 | 11621 | 11622 | 11623 | 11624 | 11626 |
| Face, ears, eyelids, nose, lips, mucous membrane | 11640 | 11641 | 11642 | 11643 | 11644 | 11646 |
Note the pattern: the last digit of each code corresponds to the diameter range within the row. This makes the table easier to memorize once you know the starting code for each location group.
How to measure for excision coding
Excised diameter formula
Let’s break that down. The formula is:
Excised diameter = lesion’s greatest clinical diameter + (margin x 2)
The margin is counted twice because it applies to both sides of the lesion. If a lesion measures 1.2 cm and requires a 0.3 cm margin, the excised diameter is 1.2 + 0.3 + 0.3 = 1.8 cm. That falls in the 1.1-2.0 cm range.
If the margin were 0.5 cm instead: 1.2 + 0.5 + 0.5 = 2.2 cm. That falls in the 2.1-3.0 cm range. One input changes, different code.
The margin trap: what most coders get wrong
The most common exam trap is reading the lesion size from the scenario and coding directly from that number. The op report may state “2.5 cm lesion” while the excised diameter, once you add margins, is 3.2 cm. Coding 2.5 cm gives you a code in the 2.1-3.0 cm range. The correct code is in the 3.1-4.0 cm range. Two adjacent columns, two completely different codes.
On the CPC exam, answer choices will typically include both codes. The question is whether you added the margins or not.
Melanoma scenarios are a specific watch point. Standard surgical margins for melanoma in situ can run 0.5-1.0 cm. A 0.8 cm melanoma with 1.0 cm margins has an excised diameter of 2.8 cm, not 0.8 cm. If you miss that and code 11600 instead of 11603, that is a four-code error. Know this pattern cold.
When to code a repair after excision
Simple closure: included
Here’s what most guides won’t tell you: simple closure after excision is not separately billable. It is included in the excision code’s global package.
The CPT guidelines are explicit on this. When an excision is followed by simple repair, you report only the excision code. The closure is bundled. You do not add a wound repair code.
On the exam, watch for language like “sutured closed,” “simple closure,” or just “the wound was closed” without any complexity qualifier. That is simple closure, that is included, you do not code it separately.
Intermediate and complex repairs: code separately
Intermediate repair means layered closure: at least one layer of subcutaneous tissue or fascia, plus the skin. Complex repair adds complicated wound configuration, debridement, or extensive undermining.
When the operative report describes layered closure, complex reconstruction, or specific complexity language, that repair is coded separately from the excision. Intermediate repairs use codes 12031-12057. Complex repairs use 13100-13160. Code the excision plus the repair, appending modifier 59 if the same anatomical site creates bundling concern.
Adjacent tissue transfer: always separate
Adjacent tissue transfer, skin flaps, and Z-plasties are always coded separately from the excision, and they are almost always the higher-value code in the pair. This includes rhomboid flap, rotation flap, advancement flap, and pedicle flap procedures.
If you see the words “flap,” “transposition,” “rotation,” or “Z-plasty” in the operative report, that is a 14000-series code plus the excision code. They do not bundle. They do not share a code. They are two separate billable services.
8 CPC exam scenarios
Scenarios 1-4: benign lesion excisions
Scenario 1. Excision of benign lesion, trunk, 1.5 cm lesion with 0.2 cm margins.
Excised diameter: 1.5 + 0.2 + 0.2 = 1.9 cm. Location: trunk. Range: 1.1-2.0 cm benign.
Code: 11402
Scenario 2. Excision of benign lesion, right cheek, 0.4 cm lesion with 0.2 cm margins. Wound sutured closed.
Excised diameter: 0.4 + 0.2 + 0.2 = 0.8 cm. Location: face. Range: 0.6-1.0 cm benign. Closure: simple, included.
Code: 11441
Scenario 3. Benign lesion, right arm, 2.0 cm lesion with 0.4 cm margins.
Excised diameter: 2.0 + 0.4 + 0.4 = 2.8 cm. Location: arm. Range: 2.1-3.0 cm benign.
Code: 11403
The trap here: 2.0 cm reads like it belongs in the 1.1-2.0 cm column (11402). But 2.8 cm does not. Adding margins is the difference between 11402 and 11403.
Scenario 4. Benign lesion, scalp, 3.5 cm lesion with 0.5 cm margins.
Excised diameter: 3.5 + 0.5 + 0.5 = 4.5 cm. Location: scalp. Range: over 4.0 cm benign.
Code: 11426
Scenarios 5-8: malignant lesion excisions
Scenario 5. Malignant melanoma, back, 0.8 cm lesion with 1.0 cm margins (standard melanoma margin).
Excised diameter: 0.8 + 1.0 + 1.0 = 2.8 cm. Location: trunk (back). Range: 2.1-3.0 cm malignant.
Code: 11603
The trap: 0.8 cm lesion reads like the 0.6-1.0 cm column (11601). The margins change everything. Melanoma scenarios on the CPC exam are almost always designed to catch this error.
Scenario 6. Squamous cell carcinoma, nose, 0.5 cm lesion with 0.3 cm margins.
Excised diameter: 0.5 + 0.3 + 0.3 = 1.1 cm. Location: face/nose. Range: 1.1-2.0 cm malignant.
Code: 11641
Not 11640 (which is 0.5 cm or less). The excised diameter of 1.1 cm puts it in the next column.
Scenario 7. Malignant lesion, left hand, 1.0 cm lesion with 0.5 cm margins. Intermediate repair performed.
Excised diameter: 1.0 + 0.5 + 0.5 = 2.0 cm. Location: hand (scalp/neck/hands group). Range: 1.1-2.0 cm malignant. Repair: intermediate, coded separately.
Codes: 11621 + 12031 (or appropriate intermediate repair code by length)
Process of elimination: once you’ve eliminated one code, the whole answer is wrong. Any answer choice showing only 11621 or only 12031 is incomplete.
Scenario 8. Basal cell carcinoma, right ear, 1.5 cm lesion with 0.3 cm margins. Flap reconstruction performed.
Excised diameter: 1.5 + 0.3 + 0.3 = 2.1 cm. Location: face/ears. Range: 2.1-3.0 cm malignant. Repair: flap, always coded separately.
Codes: 11643 + adjacent tissue transfer code (14040-14041)
The flap code is the higher-value code and is always reported separately from the excision.
Sources
- AMA CPT codebook: Integumentary System guidelines (Section 11000-11999)
- AAPC: Skin Lesion Excision coding guidance
- CMS NCCI Policy Manual: Chapter III, Surgery, Integumentary System
Test your integumentary coding: free excision quiz or work through modifier rules and NCCI bundling next. For the full picture on all 17 exam domains and how integumentary fits into your study priority order, see the CPC exam body systems guide. On the diagnosis side, the ICD-10 excludes notes guide covers how to handle comorbid diagnoses alongside a procedure code.
Sources & References
Frequently Asked Questions
Should lesion sizes be added up to report one CPT code? ▼
No. Each lesion excision is coded separately. Do not add lesion sizes together to get a larger code. Each lesion gets its own code based on its individual excised diameter, location, and pathology type.
When should a separate code for wound repair be assigned after excision? ▼
Code a separate repair only when an intermediate or complex repair is performed: layered closure, complex reconstruction, or adjacent tissue transfer. Simple closure is included in the excision code and is not coded separately.
What CPT code is used for excision of a malignant lesion from the right arm? ▼
It depends on the excised diameter (lesion plus margins). Excised diameters 0.5 cm or less: 11600. Up to 1.0 cm: 11601. Up to 2.0 cm: 11602. Up to 3.0 cm: 11603. Up to 4.0 cm: 11604. Over 4.0 cm: 11606.
What is the difference between benign and malignant excision coding? ▼
The code ranges are completely separate: benign (11400-11471) and malignant (11600-11646). Malignant lesions typically require wider margins, which affects the excised diameter calculation. The location groups and diameter breakpoints are the same for both.
Test Your Knowledge
5 quick questions on this topic.
Related Articles

ICD-10 Diagnosis Sequencing Rules: Principal vs Secondary + CPC Exam Tips
Which diagnosis goes first? ICD-10 sequencing rules for inpatient and outpatient settings, with 8 CPC exam scenarios covering principal diagnosis, comorbidities, and combination codes.

NCCI Bundling Rules: When to Use Modifier 59, XE, XS, XP, XU
NCCI edits bundle procedure codes CMS considers included in a more comprehensive code. Here is when modifier 59 and the X modifiers override a bundle: with 12 CPC exam scenarios.
ICD-10 Excludes1 vs Excludes2: Complete Coding Guide for the CPC Exam
What is the difference between Excludes1 and Excludes2 in ICD-10-CM? Here is the plain-English explanation with a decision flowchart and 10 real coding examples.
Ready to practice?
Test your CPC knowledge with real exam-style questions. Free to start.
Start Blitz Mode